Welcome to our new location in El Dorado Hills! I am excited to share my invention and new rehabilitation product SwivX within our new clinic. There is no clinic in the world that can deliver real-time functional posture analysis for both neck and back until now! What does this mean for you? I have always gone to great lengths to not only help my patients get out of pain but to help them stay out of pain. I do this by taking the time to educate my patients and explain the biomechanics involved as it relates to the mechanism of injury. I literally show patients how to stay out of my clinic which is in contrast to making people sign long contracts to get care or maybe just a “pop” and out the door. My feeling is that if you are required to sign a contract for continued care you are likely part of a business plan not a treatment plan. My approach may not be the best business plan but it is my passion to empower YOU the patient which is ultimately why I became a doctor. SwivX is a new posture tool that I designed to give my patients long-lasting and constant results with the intent to not only help their biomechanics but to also help increase spinal stability with corrective exercises within the SwivX App. Comprehensive care requires addressing mobility, stability and proper body mechanics, and SwivX provides powerful applications to help facilitate this triad of rehabilitation. It’s like having your own personal posture coach and trainer 24/7. I would like to thank all of my patients for allowing me the time and flexibility to complete this product. I guess you can call SwivX my labor of love, but I am also confident once you try it you will love it too!![]()
![]()
News
What’s causing my shoulder pain?
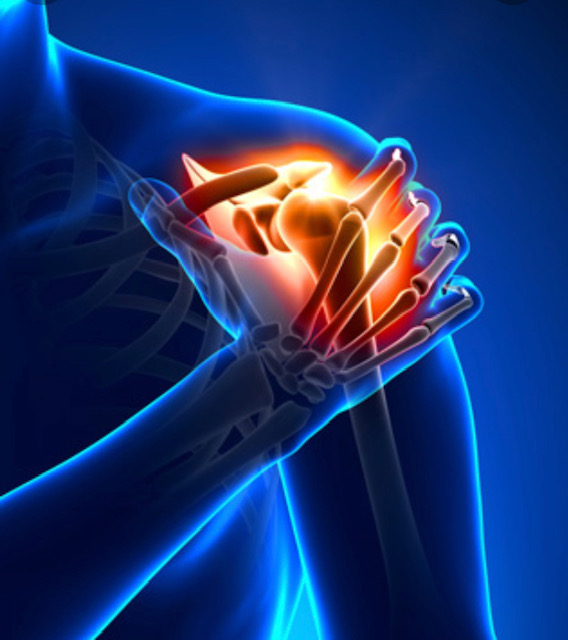
My first question when I evaluate my patient’s shoulder is… Can you sleep on your shoulder? This question helps me determine if the patient’s shoulder capsule is swollen. There are many reasons why a person develops shoulder pain but knowing the mechanism of the injury helps to narrow the diagnosis. You might injure it in a fall or accident, or you could have overdone a chore like painting. Sometimes shoulder pain comes from a condition like arthritis. If your shoulder pain started after trauma like a fall a special study might be indicated. The pain may come more gradual and then it progresses rapidly to the point of very limited motion. We sometime refer to this as frozen shoulder or medically known as adhesive capsulitis.
I often see patients develop minimal pain in the front of their shoulder as they perform task such as weight lifting. This pain may naturally subside due to slight bursa inflammation or as we call it bursitis. However, if the pain becomes worse with activity there may be slight connective tissue or scar tissue causing increase friction. The progression of symptoms for some patients can range. I have patients that develop only achiness and then it goes away for awhile and pops up from time to time.
Generally this may indication that there is mild scar tissue formation. But I also have patients that can’t move their should overnight with no real history of injury. This can be a mystery, however, I would guess that 90% of these patients did a task the day before that placed the shoulder in a compromised position. If you are noticing your shoulder pain in not going away it is important to come in and get appropriate care so that the injury does not progress into something that requires more invasive treatment options.
Personally I find that once I examine the patient and diagnosis the injury a bit of relief is seen on their face because the unknown was scary. More often than not the shoulder injury is easily resolved with applying a sports medicine protocol in just a few sessions. Although every injury has a little different presentation we can apply the concepts in a direct way to help the patient understand the mechanism of the injury as well as develop a treatment plan that is tailored for their needs. This may involve soft tissue work, ultrasound, myofascial release, electrical stimulation, cryotherapy (GameReady), and corrective exercises. If you are suffering from nagging shoulder pain don’t hesitate to make an appointment by pressing the tab above. I look for forward in helping you get back to your game!
Cryotherapy–This is how the Pros stay COOL
Game Ready is ready for you at BackBasics. Game ready was introduced to me while treating and traveling with the San Francisco 49ers. Game Ready is definitely more comfortable then standing in some Ice Chamber in subzero temperature. Extremity injuries such as ankle, knee and shoulder can be difficult to ice due to the bony articulations of the joint. Game Ready allows the operator to dial in the exact temperature and pick the desired level of compression. This system allows for a decrease in swelling and promotes faster healing time. This is just one of our sports medicine modalities that will help you get BACK to your GAME!

SAM Sport — Wearable ultrasound
 Are you ready for the latest in rehabilitative technology? Professional athletes are now using SAM Sport with their injury recovery and seeing staggering results. As a healthcare provider, I am always evaluating the latest and greatest in sports recovery and rehabilitation. I typically look at new products with a little skepticism but this product caught my eye.
Are you ready for the latest in rehabilitative technology? Professional athletes are now using SAM Sport with their injury recovery and seeing staggering results. As a healthcare provider, I am always evaluating the latest and greatest in sports recovery and rehabilitation. I typically look at new products with a little skepticism but this product caught my eye.
My approach to treating accumulative trauma injuries that result in tendonitis and other “itis” involves a therapeutic approach. This may include soft tissue or myofascial release, electric stimulation, corrective exercise and ultrasound. However, many of my patients are athletes and the last thing they want to do is stop. Having a wearable ultrasound unit enhances collagen type I and type III fibers for tissue rebuilding. Although we have only had the unit at our Folsom clinic for a short time, it is showing great results.
Why is our Healthcare Broken?
How do doctors get paid?
Imagine going to your favorite restaurant. You are greeted at the door by the hostess, who seats you and takes your drink order. You order through your favorite waiter, Andrew, who recommends the special of the day: prime rib with a dinner salad and a chocolate torte for dessert. Soon after, the food is brought out and it is delicious! You have time to enjoy your food. You then receive the bill and pay for your meal, returning to your home satisfied, all your dining needs met. Let’s say, for simplicity’s sake, you paid $75 for this meal: $50 for the steak, $10 for the salad and $15 for the dessert.
A change then occurs in the restaurant industry. A new form of eating out has been adopted. Your favorite restaurant has now contracted with over 30 different ”restaurant insurance companies.”
Anticipating another pleasant dining experience, your return to the restaurant with your new “subscribers card.” You pay your $5 “copay.” You sit in the foyer of the restaurant. You wait an hour, even though you made reservations. A harried Andrew greets you and quickly takes your order after you briefly glance at the menu. The food arrives at your table. As you take your second bite, Andrew informs you that “your time is up” and the table is reserved for another party. You are escorted outside with your hastily boxed left-overs.
What has happened to the restaurant? Behind the scenes, the restaurant owner has learned some tough realities of the “new system.” During the first month of taking insurance, the owner sends a form to the insurance company requesting payment for the $75 steak dinner: $50 for the steak, $10 for the salad and $15 for the torte. The contract with the insurance company already states that they will only pay $45 for the $50 steak, but the owner decides that the extra customers brought to the restaurant by contracting with this insurance company will more than off-set this small loss.
The first attempt at collecting the $75 dollars for the full meal is returned unpaid with the note that it was rejected due to a “coding error.” The forms for payment from the insurance company require the owner to list the parts of the meal, not by name, but by the numerical codes. The owner had listed the salad by the wrong numerical code. No suggestions for the correct code are offered, so the restaurant owner purchases a series of books, at a cost of $500, to learn how to assign the correct code to the different parts of the meals. These books will need to be bought annually due to the constant changing of the code numbers. After 30 minutes of study, the owner realizes the dinner salad should be coded as a 723.13, not the723.1 the owner originally put on the form. The salad, it turns out, needed to have two digits after the decimal point, indicating that it was a dinner salad, and not a “main course” salad. The owner mails the corrected form.
In response to the second request for payment, the insurance company does not send a check, but a detailed questionnaire: Was garlic used in seasoning the steak? Was it necessary to use garlic for this particular recipe? Did the restaurant ask for permission to use garlic from the insurance company before serving the steak? Why was salt, a less expensive alternative, not used instead? The owner submits the answers, emphasizing that the garlic is part of a secret family recipe that made the restaurant famous.
The owner waits another week (it has now been 3 weeks since the dinner was served). The check arrives three and a half weeks after the meal was served. The check is for $20 and states that it is specifically for the steak. The check also comes with a letter stating that no billing of the patron may occur for the salad, but no other explanation is enclosed. No mention is made of the $15 dessert.
The now frustrated restaurant owner calls the provider service number listed in the contract. After five separate phone calls to five different numbers (The harried voice behind phone call number four explains that the insurance company has merged with another insurance company and the phone numbers had all changed last week, sorry for the inconvenience…), the owner gets to ask why, when the contract says the steak will be paid at $45, has the check only been written for $20? And what happened to the payment for the $10 salad and the $15 dessert?
As it turns out, this particular patron’s insurance contract only pays $45 when the patron has reached their deductible, which this patron has not at this time. The remaining portion of payment for the steak must now be billed by the restaurant to the patron directly.
The $10 for the salad would have been paid if the patron had ordered it on a different day, but, per page 35 in the contract, because it was billed on the same day as the steak, it is considered to be part of the payment for the steak and no extra money can be collected from the patron or the insurance company.
The dessert, the owner learns, should have had a “modifier” number put with its particular billing code when billed with the steak and the salad.
Realizing that the insurance billing is quite a bit harder than anticipated, the restaurant owner hires a company, who is paid 5% of any money collected to specifically make sure these coding errors do not occur again and follow up on payment rejections. For an additional $99 per month, the billing company will “scrub” the forms submitted for payment to make sure specific clerical errors will not cause future delays in payment.
The owner now must lay off the hostess and the bus boy to pay the billing company, so these duties are now added to the waiter’s other responsibilities.
In the meantime, the restaurant owner has also had the waiter take on the job of answering the phones due to the now high volume of phone calls from patrons questioning why they are receiving bills for meals they ate over two months ago, and why did their insurance company not pay for this portion of the meal? This extra work is now resulting in longer times patrons must wait to be seated, and grumblings from the waiters who “were not hired or trained to do this kind of work.”
The owner now realizes that, although the dinner originally cost $75 to make, only $25 has been paid. The remaining $30 billed to the patron is now in its third mailing, with the first two requests for payment going unanswered by the patron. The restaurant owner realizes a collection agency must be employed in order to have any hope of receiving any portion of payment from the patron.
Each meal served now costs at least an additional $20 due to the added overhead of the billing company, coding books, and the collection agency. These added expenses have nothing to do with cooking food or providing any direct service to the restaurant’s customers.
Service to the restaurant’s patrons has been compromised with these changes as well. The owner has now over-extended the waiter, who was an excellent waiter, but is now taking on the roles of host, phone answering and table bussing.
In order to even meet the costs of providing fine dining, the restaurant owner now must seat twice as many patrons in the same amount of time.
What was once an outstanding business that focused on fine dining and customer service has now been turned into a business in the business of trying to get paid.
Alas, I wish this were a fictional tale, but it is not. The only fictional portion is that this is not your favorite restaurant, but your favorite doctor’s office, which is responsible not for meeting your dining needs, but those of your health.
Megan Lewis, M.D.
A family physician in rural Colorado.
This story will explain the problem. Just view this ://idealmedicalpractices.typepad.com/ideal_medical_practices/2009/02/health-insurance-for-all-is-great-but-not-enough-to-solve-the-problem.html
Where is my back pain coming from?
I can remember my first patient in clinic many years ago. I tried to explain everything I knew about the spine and their injury. The patient looked at me like a deer caught in the headlights. I could tell they were listening but I was unaware that I was just spewing out all these fancy medical terms that had been crammed down my throat in chiropractic school. It took me a few “headlights” to learn how to bring my education to the patient in a manner that they could understand. In someways this took more skill to master than learning all those fancy medical terms.
When discussing the spine I have found that it is important to break down the pain generator components. Most patients associate pain as their problem. It can be difficult to explain that pain is not the problem, but a symptom of the problem. Confused? Well, you would not be the only one. Understanding spinal injuries takes a complete view of the musculature and neurological systems. It is possible to break the complexity of the these systems into three pain generators.
The first pain generator can relate to the facet joint. This pain generator is generally lower on the pain scale. There are orthopedic test to ascertain the presents of irritation of this joint. I say “generally” lower pain but I have seen these joints become very painful with some high impact football injuries and auto injuries.
The second pain generator may be due to an annular disc injury. These injuries can be deceptive with pain going down the back of the legs and arms. Many patients may not even present with lower back pain but they have significant leg pain. Now try to convince the patient they have a back problem when they are coming in with zero back pain. This is what exemplifies the meaning of pain is the symptom and not source of the problem.
The third pain generator may relate to the spinal nerve that exits at the disc level. This nerve may become irritated from the inflammation caused by a disc injury or may become impinged by the disc or a degenerative process. Orthopedic test can determine what type of impingement the patient is dealing with.
Although I still continued to use these dreaded medical terms….we can break in down into three simple terms
- Facet
- Disc
- Nerve
If you are continuing to suffer from reoccurring lower back or neck pain, come in an see how to take control of your symptoms. My clinical treatments are based on rehabilitation and not just a “pop” and out the door you go. Come see what you are missing.
John Pellegrini, D.C.